 | ||||||||||||||||||
| STUDI E RICERCHE SPECIFICHE | ||||||||||||||||||
|
Increased Carrying Reduces Infant Crying: A Randomized Controlled Trial Urs A. Hunziker, MD, and Ronald G. Barr, MDCM, FRCP(C) From the Department of Pediatrics, The McGill University-Montreal Children's Hospital Research Institute, Montreal, Quebec, Canada. ABSTRACT. The crying pattern of normal infants in industrialized societies is characterized by an overall increase until 6 weeks of age followed by a decline until 4 months of age with a preponderance of evening crying. We hypothesized that this "normal" crying could be reduced by supplemental carrying, that is, increased carrying throughout the day in addition to that which occurs during feeding and in response to crying. In a randomized controlled trial, 99 mother-infant pairs were assigned to an increased carrying or control group. At the time of peak crying (6 weeks of age), infants who received supplemental carrying cried and fussed 43% less (1.23 u 2.16 h/d) overall, and 51% less (0.63 u 1.28 hours) during the evening hours (4 PM to midnight). Similar but smaller decreases occurred at 4,8, and 12 weeks of age. Decreased crying and fussing were associated with increased contentment and feeding frequency but no change in feeding duration or sleep. We conclude that supplemental carrying modifies "normal" crying by reducing the duration and altering the typical pattern of crying and fussing in the first 3 months of life. The relative lack of carrying in our society may predispose to crying and colic in normal infants. Pediatrics 1986;77:641-648; crying, carrying, colic,- mother-infant interaction. All normal infants cry. In our society, crying typically occurs in a pattern characterized by an increase in crying duration until about 6 weeks of age, followed by a gradual decrease until 4 months of age.1'4 Within the day, crying is increasingly prevalent during the late afternoon and evening hours.1'2'4'5 Although we have come to regard this crying pattern as "normal,"!'6 infants with similar crying patterns are frequently brought to pediatric clinicians as crying problems. Not uncommonly, they are labeled as having "paroxysmal fussing" or "3-month colic,"1'2'7"9 variously estimated to affect about 20% of normal newborns.2'9'10 In recent years, crying has come under increasing scrutiny, not only because of its theoretical importance in early mother-infant interaction,11'14 but also because of its clinical importance as a cause of maternal distress,12 a cause of discontinuation of breast-feeding,5 and a stimulus for child abuse. METHODS Overall Design The study was a randomized controlled trial to assess the effectiveness of supplemental parental carrying in reducing crying/fussing behavior of normal infants between 3 and 12 weeks of age. Normal mother-infant pairs were recruited at birth and entered the trial when the baby was 3 weeks of age. After obtaining baseline data for 1 week, subjects were randomized to a supplemental carrying or control group. In the supplemented group, parents were asked to carry their baby in their arms or in a carrier for at least three hours a day. In the control group, parents were asked to situate their baby facing a mobile and an "abstract" of a face when the baby was placed in the crib. Infant behaviors, including crying and fussing, and parental activities directed toward the infant were monitored by diaries completed by the parent(s) at week 3 (baseline) and when the baby was 4, 6, 8, and 12 weeks of age. The study was approved by the Montreal Children's Hospital Committee on Medical and Dental Evaluation and all participating mothers gave written informed consent. Subjects Between June and November 1983, 234 eligible mother-infant pairs were approached on maternity wards of two general hospitals in central Montreal. AU infants eligible for the study were breast-fed, first-born at term with a birth weight of at least 2,500 g and had uncomplicated pre-, peri-, and postnatal histories. The nature of the trial was explained and they were told that, if they participated, the form of additional stimulation (carrying or visual) they would be asked to provide would be determined randomly (by chance). Of those who were eligible, 50% (n = 117) agreed to participate at 3 weeks. By randomization, 59 babies were assigned to the supplemented group (ten subsequently dropped out); 58 were assigned to the control group (eight left the study). Reasons given for discontinuation were maternal inconvenience (n = 11), including the work of completing diaries regularly (missing 2 weeks or more), being too busy, and maternal illness; infant illness (n = 1); and miscellaneous (n = 6), including diaries lost in the mail and change of residence. Subjects who discontinued the study differed from those who remained: those who left were of lower socioeconomic status (61 o 68 by Green Index,35 unpaired t = 3.02, P < .01) and younger (26 u 29 years, unpaired t = 2.68, P < .01) but they were not different on neonatal indices (duration of gestation, birth weight, Apgar score at one and five minutes), infant characteristics (sex, race) and remaining parental characteristics (religion, language, marital status, age of father). In the remaining 49 supplemented and 50 control subjects, there were no differences on any of the above infant or parental variables (Table). Size of this study population was determined a priori on the assumption that a reduction of 25% in daily crying/fussing behavior would be a meaningful behavioral change. We used previously available data36 to determine that a sample size of 45 subjects per group would be sufficient for a decrease of this magnitude to occur by chance in only 5% of samples, whereas a true decrease would fail to be seen in 20%. For some subjects, 1 week of diary data was missing, but missing data never exceeded 10% of the total for either group for any week. Parental Diaries Parents recorded their baby's behaviors and their own activities in pretested continuous 24-hour diaries. One complete day was represented on each sheet by four horizontal "time" bars, each subdivided into five-minute units. The upper half of each bar was used for recording infant behaviors of sleeping, awake and content, crying, fussing, and feeding. The lower half was used for recording parental activities of carrying with body contact, moving with the baby but without body contact (ie, in a car or a pram) and care-taking activities (ie, changing, bathing, dressing the baby). The duration of each behavior was indicated by filling in these bars with a symbol assigned to each behavior. The diaries of the supplemental and control groups differed only in the name given to the symbol representing the intervention. For the baseline recording (week 3), this category was omitted for both groups. | ||||||||||||||||||
 The dependent measures of infant behavior derived from the diaries were duration (hours per day) and frequency (episodes per day) of crying/fussing (crying and fussing combined), sleeping, awake and content, and feeding. The same measures were derived for parental activities of carrying with body contact, moving baby without body contact, and care taking. These measures were also derived for three periods of the day: night (midnight to 8 am), day (8 AM to 4 PM) and evening (4 PM to midnight). To monitor potential recording bias introduced by the different interventions, parents also recorded the frequency of five infant behaviors presumed not to be affected by parental carrying, specifically hiccups, bowel movements, regurgitation, vomiting, and tremors. Procedure At the time of recruitment, eligible mothers were provided with the diary and verbal and written instructions regarding its use. At week 3, parents were contacted by telephone to determine whether they wished to be study participants. Participating parents were then asked to complete the diary for 1 week. At the end of week 3, parents were assigned by random number to the supplemented or control group, and they were then visited at their homes. Diaries were reviewed and new diaries were provided for the remainder of the study. In the supplemented group, parents were asked to carry their baby for a minimum of three hours per day and it was emphasized that carrying should occur throughout the day, not only in response to crying, in addition to carrying during feeding, and independent of whether the baby was awake or asleep. In the control group, parents were asked to expose their infant to the visual stimuli when they were placed in the crib, but they were not asked to increase time in the crib. The investigators provided infant carriers to the supplemented group and mobiles and face pictures to the control group. To minimize recording bias, the purpose of the study was described as being the study of the effect of additional amounts of common stimulation on the development of behavioral rhythms (sleep, feeding, regurgitation, etc) in normal infants. Neither the specific hypothesis nor the crying target variables (crying and fussing) were identified to the parents. During weeks 4 to 12, the parents were contacted by telephone at the beginning of each week scheduled for diary recording. Completed diaries were returned by mail after each week of recording. At the end of week 12, parents were asked about the type of current feeding (breast, formula, mixed) and whether the pacifier had been used frequently or rarely. Data Analysis A research assistant blind to the study hypothesis transferred the parental recordings of each diary sheet to an identical diary analogue displayed on the screen of a computer terminal. Compilation of frequencies and duration of behaviors, data reduction, and analyses were accomplished by programs developed for this study. Between-group differences were analyzed by planned comparisons using Student's one-way t test of the means of independent samples.
 Fig.1 |
Daily duration of infant crying/fussing in re-sponse to change in parental carrying. Top: Means and SD of crying/fussing behavior in hours per day averaged over each week of parental recording for supplemented (0, - - -) and control (o, --) infants, respectively. Intervention (see text) for both groups started at begin-ning of week 4 after 1 week of baseline recording (week 3). Bottom: Means and SD of carrying in hours per day averaged over each week of parental recording for sup-plemented and control groups. Carrying during interven-tion in supplemented group is represented by method of holding in parent's arms or in infant carrier.
| RESULTS As expected, the mean daily duration of carrying of supplemented and control infants was similar during week 3 (3.4 y 2.7 h/d, P > .05; Fig 1, bottom). At each of weeks 4 to 12, parents in the supplemented group did significantly more carrying, the difference ranging from 2.1 h/d at week 4 to 1.5 h/ .-d at week 12 (average 1.8 h/d; all P < .001). As a result, the supplemented infants were carried an average of 4.4 h/d during the intervention period, of which 3.5 hours was in the parent's arms and 0.9 hours was in the carrier. The control infants were carried an average of 2.7 h/d throughout this intervention period. 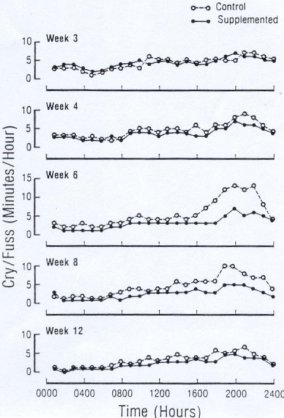 Fig.2 |
Distribution of infant crying/fussing behavior within day. Mean crying/fussing behavior in minutes per hour at each hour of day for supplemented and control infants during baseline (week 3) and during weeks 4, 6, 8, and 12 of the intervention period.
The typical clustering of crying during the evening remained the same for both groups at all ages. However, although the supplemented group tended to have less crying/ fussing behavior throughout the day, these differences were particularly striking during the evening, representing a reduction of 54% and 47% at weeks 6 and 8, respectively. Significant reductions within the day occurred at week 6 during the day (0.4 u 0.6 hours, P < .005), evening (0.6 u 1.3 hours; P < .005), and night (0.2 u 0.3 hours; P < .01). At week 8, significant reductions occurred during the day (0.4 v 0.6 hours; P < .001) and evening (0.5 v 1.0 hours; P < .001). There were no significant differences within the day during weeks 4 and 12. | To determine which other behaviors may have been affected, similar analyses were performed post hoc for feeding, sleeping, and awake and content duration. There were no differences in feeding or sleeping duration at any age; however, awake and content behavior was significantly increased in the supplemented babies at weeks 4 (4.1 u 3.8 h/d), 6 (5.6 u 4.6 h/d), and 8 (6.0 u 5.0 h/d; all P < .01). It appeared, therefore, that reduced crying/fussing was replaced by increased awake and content behavior during this time. During the intervention period, the feeding frequency calculated in mean episodes per day was higher in the supplemented compared with the control group, averaging 8.8 u 7.2 episodes per day (P < .025 at all weeks). This was in contrast to the frequency measures calculated for all other infant behaviors (crying/fussing, sleeping, feeding, awake and content) which were similar in both groups during all weeks. In addition, there were no between-group differences in frequency of hiccups, bowel movements, regurgitation, vomiting, or tremors. With respect to the retrospective question concerning pacifier use, frequent use was reported by 70% of the control parents o 47% of the parents of supplemented babies (x2 = 5.15, P < .05). Forty-five percent of supplemented and 40% of control parents reported having introduced partial or total formula feeding by the end of the study period (P > .05). DISCUSSION The results of the present study demonstrate that increased parental carrying was associated with a substantial reduction in crying and fussing behavior in these first-born, breast-feeding infants during the first 3 months of life. This behavioral change was particularly apparent in relation to two of the characteristics of crying of normal infants noted in our control group and in previous studies namely, elimination of the peak at 6 weeks of age and diminution of the crying and fussing that clusters during the evening. This reduction appeared to be replaced by increased awake contentment rather than changes in sleeping or feeding duration. The difference was most marked by 6 weeks of age when an increase in carrying time of two hours was associated with an overall reduction of one hour (43%) in crying and fussing behavior. Whether these findings can be generalized to bottle feeders, later parity infants, infants with younger mothers and lower socioeconomic status, or mother-infant pairs who choose not to participate in such studies cannot be determined from this study. SPECULATION AND RELEVANCE The rather impressive change implies that this pattern of crying in the first 3 months of life is only normal in the sense of being typical for infant care-giving practices of our society. However, these findings do not demonstrate that absence of carrying is either a necessary or a sufficient cause of infant crying. It is probable that this particular pattern reflects underlying biologic changes, the behavioral manifestations of which are subject to modulation by different care-taking practices. For example, the changes in crying may represent changes in development and maturation of the nervous system facilitated by favorable interaction with the care-taking environment.1'3'14 Additionally, crying and fussing could be initiated by the stimulus of intraintestinal gas production secondary to the incomplete carbohydrate absorption which persists into the third month of life in response to typical feeding patterns.36'43 Whatever the particular constraints imposed by these biologic factors, the behavioral manifestations nevertheless remain subject in part to environmental influence. Consequently, normal crying most likely represents a culture-specific pattern reflecting the interaction between biologic factors and infant care-giving practices typical of our society. We speculate that the potential for changing infant-carrying patterns may have important clinical consequences. Early infant crying is an adaptive behavior that acts to promote mother-infant proximity and to provide opportunities for social interaction.11'14 These opportunities usually result in elicitation of appropriate emotional-motivational reactions, care and feeding behavior, and parent-child attachment.3'11'12 The increased carrying reduces crying behavior but promotes proximity so that crying is less necessary. In addition, the associated increased awake contentment would likely be associated with a state of quite alertness and visual exploration necessary for positive social contact.25'30 If an infant's crying behavior is considered excessive, however, it may promote negative interactions12 and increase the frequency of clinical complaints. Excessive crying has been associated with the erosion of positive emotions and coping skills in mothers,44'45 parental responses that are less plentiful and of poorer quality,46 and occasionally episodes of child abuse.ls'16 In clinical practice, complaints of crying typically present as feeding problems or as colic. Because parents commonly perceive crying as hunger, elimination of the crying peak may remove one impetus to engage in formula changes, discontinue breast-feeding, or begin early solid food intake.5'47 Indeed, the associated increased feeding frequency noted with the carried infants might also facilitate early weight gain, prolong breast-feeding, and diminish the insufficient milk syndrome in breast-feeding infants.48'49 Finally, increased carrying, particularly anticipatory carrying throughout the day, may represent a relatively simple nonpharmacologic therapeutic intervention for colic, because there is a close similarity between the patterns of crying seen in normal babies and infants with colic, as well as lack of evidence of pathology in colicky infants.2'7'9 Alternatively, increased carrying may have significance as part of pediatric anticipatory guidance. Overall, supplemental carrying may be a more effective approach to feeding and crying problems than the more traditional supplemental bottle. ACKNOWLEDGMENTS This study was supported, in part, by grants from the McGill University-Montreal Children's Hospital Research Institute and the W. T. Grant Foundation. REFERENCES 1. Brazelton TB: Crying in infancy. Pediatrics 1962:29:579-588 2. Wessel MA, Cobb JC, Jackson ES, et al: Paroxysmal fussing in infancy. Pediatrics 1954:14:421-434 -� 3. Erode RN, Gaensbauer TJ, Hannon RJ: Emotional Expression in Infancy: A Biobehauioral Study. New York, International University Press, 1976, pp 80-85 4. Rebelsky F, Black R: Crying in infancy. J Genet Psychol 1972:121:49-57 5. Bernal J: Crying during the first ten days of life. Dev Med Child Neurol 1972:14:362-372 6. Bax M: Clinical analysis of the cry. Deu Med Child Neurol -1975:17:799-801 7. Paradise JL: Maternal and other factors in the etiology of infantile colic. JAMA 1966:197:123-131 8. Illingworth RS: "Three months colic." Arch Dis Child 1954:29:165-174 9. Meyer JE, Thaler MM: Colic in low birth weight infants. Am J Dis Child 1971:122:25-27 10. Hide DW, Guyer BM: Prevalence of infant colic. Arch Dis Child 1972:57:559-560 11. Bell SM, Ainsworth DS: Infant crying and maternal respon-siveness. Child Deu 1972:43:1171-1190 12. Murray AD: Infant crying as an elicitor of parental behavior: An examination of two models. Psvchol Bull 1979:86:191-215 13. Thoman EB, Acebo C, Becker PT: Infant crying and stability in the mother-infant relationship: A system analysis. Child Dev 1983:54:653-659 14. Lester BM, Zeskind PS: A biobehavioral perspective on crying in early infancy, in Fitzgerald HE, Lester BM, Yog-man MW (eds): Theory and Research in Behavioral Pediatrics. New York, Plenum Press, 1982, pp 133-180 15. Frodi AM: Contribution of infant characteristics to child abuse. Am J Ment Defic 1981:85:341-349 16. Steele B, Pollack C: A psychiatric study of parents who abuse infants and small children, in Heifer R, Kempe C (eds): The Battered Child. Chicago, University of Chicago Press, 1968, pp 89-133 17. Brazelton TB, Robey JS, Collier GA: Infant development in the Zinancanteco Indians of southern Mexico. Pediatrics 1969:44:274-283 18. Goldberg S: Infant care and growth in urban Zambia. Hum Dev 1972:15:77-89 19. Konner MJ: Aspects of the developmental ethology of a foraging people, in Blurton-Jones NG (ed): Ethological Studies of Child Behavior. Cambridge, Cambridge University Press, 1972, pp 285-304 20. Mead M: Sex and Temperament in Three Primitive Societies. London. Routledge & Kegan Paul, 1935 21. Ainsworth DS: Infant development and mother-infant interaction among Ganda and American families, in Leider-man PH, Tulkin SR, Rosenfeld A (eds): Culture and Infancy: Variations in the Human Experiences. New York, Academic Press, Inc, 1977, pp 119-149 22. Koroer AF, Grobstein R: Visual alertness as related to soothing in neonates: Implications for maternal stimulation and early deprivation. Child Deu 1966:37:867-876 23. Korner AF, Thoman EB: Visual alertness in neonates as evoked by maternal care. J Exp Child Psvchol 1970:10:67-78 24. Korner AF, Thoman EB: The relative efficacy of contact and vestibular-proprioceptive stimulation in soothing neonates. Child Dev 1972:43:443-453 25. Gregg CL, Haffner ME, Korner AF: The relative efficacy of vestibular-proprioceptive stimulation and the upright position in enhancing visual pursuit in neonates. Child Dev 1976:47:309-314 26. Thoman EB, Korner AF, Beason-Williams L: Modification of responsiveness to maternal vocalization in the neonate. Child Dev 1977:48:563-569 27. Bims B, Blank M, Bridger WH: The effectiveness of various soothing techniques on human neonates. Psvchosom Med 1966:28:316-322 28. White BL, Castle PW: Visual exploratory behavior following postnatal handling of human infants. Percept Mot Skills 1964:18:497-502 29. Van den Daele LD: Modification of infant state by treatment - - in a rockerbox. J PsycAo^ 4970:74:161-165 30. Fredrickson WT, Brown JV: Posture as a determinant of visual behavior in newborns. Child Deu 197o;46:o79-582 31. Pedersen, DR, Ter Vrugt D: The influence of amplitude and frequency of vestibular stimulation on the activity of two-month-old infants. Child Deu 1973:44:122-128 32. Ter Vrugt D, Pedersen DR: The effects of vertical rocking frequencies on the arousal level in two-month-old infants. Child Deu 1973:44:205-209 33. Pedersen DR: The soothing effect of rocking as determined by the direction and frequency of movement. Can J Behau Sci 1975:7:237-243 34. Wolff PH: The natural history of crying and other vocalizations in early infancy, in Foss BM (ed): Determinants of Infant Behavior. IV. London, Methuen. 1969, pp 81-109 35. Green LW: Manual for scoring socioeconomic status for research on health behavior. Public Health Rep 1970:85:815-827 36. Barr RG, Hanley J, Palterson DK: Does incomplete lactose absorption predispose to crying in normal infants? abstracted. Soc Res Child Deu Program 1983:4:12 37. Barr RG, Kramer MS, Leduc DG, et al: Validation of a parental diary of infant cry/fuss behavior by a 24-hour voice-activated infant recording (VAR) system. Program Ambulatory Fed Association 1982, p 69 38. Sander LW, Stechler G, Burns P, et al: Early mother-infant interaction and 24-hour patterns of activity and sleep. J Am Acad Child Psychiatry 1970:9:103-123 39. Brackbill Y: Cumulative effects of continuous stimulation on arousal level in infants. Child Deu 1971:42:17-26 40. Brackbill Y: Continuous stimulation reduces arousal level:Stability of the effect over time.Child Dev 1973:44:43-46 41. Gordon T, Foss BM: The role of stimulation in the delay of onset of crying in the newbora infant. Q J Exp Psvchol 1966:18:79-81 42. Ourth L, Brown KB: Inadequate mothering and disturbance in the neonatal period. Child Deu 1961:32:287-295 43. Barr RG, Hanley J, Patterson DK, et al: Breath hydrogen excretion in normal infants in response to usual feeding patterns: Evidence for "functional lactase insufficiency" beyond the first month of life. J Pediatr 1984;104:527-533 44. Korner AF: Individual differences at birth: Implications for child care practices. Birth Defects 1974:10:51-61 45. Shaver BA: Maternal personality and early adaptation as related to infantile colic, in Shereslefsky P, Yarrow LJ (eds):Psychological Aspects of a First Pregnancy and Early Post-na'tal Adaptation. New York, Raven Press, 1979, pp 209-215 46. Shaw C: A comparison of the patterns of mother-baby interactions for a group of crying, irritable babies and a group of more amenable babies. Child Care Health Deu 1977;3:1-12 47. Bloom K, McDowell EE: Time-sampling caretaker and infant behaviors in the first five weeks of life. J Psychot 1972;80:111-120 48. De Carvalho M, Robertson S, Friedman A, et al: Effect of frequent breast-feeding on early milk production and infant weight gain. Pediatrics 1983;72:307-311 49. Illingworth RS, Stone DGH, Jomett GH, et al: Self-demand feeding in a maternity unit. Lancet 1952; 1:683-687
ON REMODELING SOCIETY ... even if we were determined to, we could never, despite our dreams of [a perfect society], sweep everything away and begin again. Mankind is like the crew of a ship at sea who can choose to remodel any part of the ship they live in, and can remodel it entirely section by section, but cannot remodel it all at once. Submitted by Student From Magee B: Philosophy and the Real World. An Introduction to Karl Popper. La Salle, IL, Open Court, 1985. Copyright 1986 by the American Academy of Pediatrics - Published in PEDIATRICS Vol.77, pages 641-648, No.5 May 1986 Pubblicato su www.portareipiccoli.it con il gentile permesso dell'autore Dott. Urs A.Hunziker, agosto 2002
 PERCHE' |
COME |
CHI SONO |
progetto e realizzazione: Esther Weber 2002-2010.Tutti i diritti riservati. | Colophon & Copyright | ||||||||||